
Clinical Researcher—December 2017 (Volume 31, Issue 6)
PEER REVIEWED
Rebecca Namenek Brouwer, MS; Deborah Hannah, BS; Christine Deeter, BS; Betsy Hames, JM; Denise Clutter Snyder, MS, LDN, RD
[DOI: 10.14524/CR-17-0040]
Bringing scientific discoveries to bear as safely and efficiently as possible is the goal of those involved in clinical research. To accomplish this, a skilled and stable workforce is critical—this means retaining staff who understand best practices, regulations, and how best to get things done. With today’s tight labor market, however, attracting the best and brightest to the profession of clinical research may be as challenging as retaining skilled employees.
Academic medical centers (AMCs) may experience particular challenges in recruiting high-quality staff, given the general decline of clinical research activities in this venue.1 Therefore, it’s important to create a clinical research workforce system within AMCs that appeals to potential job candidates as well as valuable incumbents, and that serves an ever-changing industry by emphasizing and rewarding development of specific competencies.
This paper describes an initiative that created a competency-based staffing structure at an AMC to provide, or at least encourage, the following:
- Standardized research roles
- A consistent approach to hiring and evaluating employees
- Advancement opportunities that rely on demonstrated competencies
- A transparent pathway for career growth and skill development
This workforce initiative was funded in part by an institutional Clinical and Translational Science Award (CTSA) grant from the National Institutes of Health (NIH) (UL1TR001117) to Duke University Medical Center. As such, it is the authors’ desire to share their experiences with others who may benefit from the work.
Background
Most adults need to work to earn a living; however, each individual has his or her own reasons for being attracted to, and remaining at, a particular job. This likely comes down to what motivates them, and many theories provide explanations for how this affects employee behavior.2
Champagne and McAfee3 offered an employee motivational theory that listed five important aspects of satisfying employee needs: physiological, security (economic, psychological, etc.), affiliation (encouraging social interaction), esteem (job challenge), and self-actualization. These needs are based on the well-known hierarchy of needs, articulated by Abraham Maslow.4
Meanwhile, the equity theory of motivation, determined by John Stacey Adams,5 invites additional factors that motivate employees. Here, staff motivation is dictated by whether they think what they are putting into a job relates to what they get out of it. Similarly, it is important that what a staff member gets out of the job is the same as his or her colleague—fair, consistent treatment is key to the equity theory.
To build and maintain a clinical research workforce within an AMC setting, Duke employed strategies to affect motivation at several levels. In this article, the authors explain the various components of the workforce initiative, which aimed to recruit, train, and retain valuable staff and bolster professionalism in clinical research support.
Setting Up a Successful System
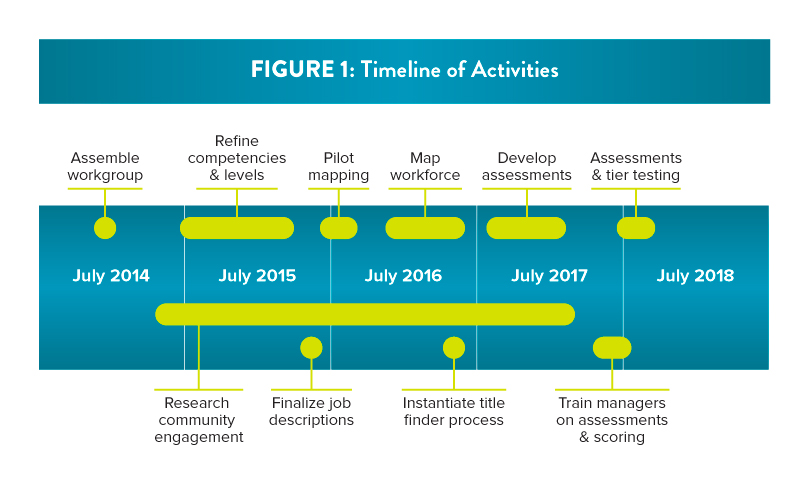
Since July 2014, Duke has been working on professionalizing its clinical research workforce via a comprehensive initiative that involves many elements (see Figure 1 for a timeline of related activities).6,7 At its core, the initiative utilizes core competencies, developed by the Joint Task Force for Clinical Trials Competency (JTFCTC).8 The eight competency domains are: (1) Scientific Concepts and Research Design, (2) Ethical and Participant Safety Considerations, (3) Medicines Development and Regulation, (4) Clinical Trial Operations (GCPs), (5) Study and Site Management, (6) Data Management and Informatics, (7) Leadership and Professionalism, and (8) Communication and Teamwork. The work was undertaken by the Clinical Research Professionals Working Group (CRPWG), comprised of staff from Duke’s School of Medicine, the Duke Office of Clinical Research,9 and the university’s Human Resources and Rewards and Recognition units.
Importantly, this initiative was heavily supported by leadership within the School of Medicine and the Human Resources unit, and it has had implications throughout the institution.
Standardizing Research Roles
The standardizing of research roles was made possible by the development of competency-based job descriptions and incumbent alignment with those job descriptions. The number of job classifications held by clinical research staff at Duke had become difficult to manage and impossible to track. In order to create consistency and standardization across the institution, the CRPWG aimed to consolidate and simplify the number of clinical research job classifications. As result of this project, the number of classifications was reduced from approximately 80 to 12.6
A tool was created to assess the current job duties and competencies of clinical research staff at Duke. The competencies were founded in the work done by the aforementioned JTFCTC, and were tracked in alignment with an initiative undertaken by the 61 institutions participating in the NIH CTSA program at the time.
Each staff member was asked to complete a survey tool, designed for collection in REDCap™ (Research Electronic Data Capture; https://www.project-redcap.org),10 based on the job duties and level of identified competencies. The staff member’s manager reviewed the tool, then validated and altered as needed the responses based upon his or her assessment of the employee’s job duties and level of competency.
The answers provided by the staff member and manager were assessed by committee, in conjunction with review of the staff member’s CV and job description. The job classification that was deemed the “best fit” was provided to the leadership of the staff member’s research unit to ensure there were no major concerns regarding the position identified. More than 700 research professionals were mapped into these new classifications in two distinct waves.
Consistent Hiring Practices
The competencies that were utilized to map each of the incumbents into their new job classifications were modified for use in a REDCap™ tool for new hires. The survey requires hiring managers to answer a series of questions based on the competencies needed to meet the requirements of the open position. Outcomes of the survey are then analyzed by a group of subject matter experts to provide the job classification that most closely aligns with the position being discussed.
Once the best fit has been identified, the results are recorded in a database and a position-specific job description is sent to the hiring manager. Communication and collaboration with the Human Resources unit ensures all positions that may fit into one of the 12 clinical research job classifications are routed through the survey tool. By utilizing this systematic method, the time to classify and post a position has been reduced significantly.
Tier Advancement
More than 40 competencies for staff in these tiered positions were leveled into four categories—”fundamental,” “skilled,” “advanced,” and “expert.” Multimodal, standardized assessments were developed for each competency, to determine the candidate’s level of skill/knowledge. Core, required competencies were identified for each role. Points were assigned for each level, and the accumulated point total determines advancement to the next tier. (It is important to note that competencies in the domain of Leadership and Professionalism play a key role.)
Through the tier advancement process, staff are able to clearly see opportunities for growth and development. This relies on the staff being able to exhibit competency in the skills required to perform their job. Staff are evaluated on these competencies by completing the previously mentioned assessments.
While an employee and his or her manager can select from several competencies, the Leadership and Professionalism competencies are required in order to progress. This fosters a sense of collaboration, professional growth, and innovation throughout the clinical research community.
The tools developed for the tier advancement process can be modified and used for training and onboarding purposes. The utilization of these tools for new hires creates consistency and efficiency across a variety of therapeutic areas of research and enhances a culture of professionalism.
While Duke has done much to professionalize its workforce, additional initiatives are in the planning stages, which will allow the institution to continue to build upon the competency model created. An example of this is that each employee who completes a competency assessment will have access to an individualized profile that reflects areas of strength within each domain. This can serve as part of an employee’s portfolio, and can be shared within the institution, as the assessments are consistent across units.
Portfolios may provide other AMCs information about research capability for staff who need to relocate and wish to continue their work at the same level. In addition, the hope is to take the competencies for each job classification and weave them into Duke’s clinical research training program and performance management system. By continuing to harmonize the expectations of managers across units, the institution aims to ensure consistent professional standards.
Discussion
This project was a significant undertaking, with regard to both time and money. Numerous staff and stakeholders were involved across the institution over several years. A core group of individuals were paid for the effort they devoted to operationally administer this initiative, but countless others volunteered their time to make it possible.
Many champions across the institution socialized the idea that the provision of career development opportunities to research professionals aims to positively affect not only individual staff, but also the institution and clinical research at large. There was some resistance to change, and concern about the financial impact shouldered by individual departments and research investigators. However, the strong commitment from the School of Medicine, Duke University Human Resources, and the research community in general made this project possible.
Stakeholder engagement in a project of this magnitude is absolutely necessary for success. The faculty were involved through their participation in an assembled Faculty Advisory Committee representing a number of clinical department disciplines, and are actively conducting their own research supported by diverse clinical research professional support teams. Their input and willingness to involve their staff in the “pilot” phase was critical.
The managers of the staff involved were also deeply engaged in this process. Manager involvement was important because managers recognized the work being done by staff, understood the expectations of each job classification, and were familiar with the specific competencies involved in each job classification. They were also called on as subject matter experts throughout the process. There were several training opportunities for these managers as the project moved along, which was key to its success and to staff understanding of the advancement opportunities.
The job classifications that were developed for clinical research staff rely on the idea of competencies being “building blocks.” The staff at a higher tier are expected to have attained their current tier’s expectations as well as the competencies of those at a lower tier. As an example of this for data entry and collection, a “fundamental” employee would be able to collect data according to a predefined plan; an “advanced” employee would not only be able to collect data according to a predefined plan, but is likely to be leading the development of standard operating procedures utilized to collect data.
The tier advancement process is point-based, and is consistent across all tiered job classifications. The institution requires the employee to meet a standardized threshold at each tier; “fundamental” requiring at least nine points, “skilled” requiring at least 36 points, and “advanced” requiring at least 84 points. Employees can achieve this threshold in many different ways. This allows for growth in areas that will fit staff who have specialties and those who may be a “jack of all trades.” Utilizing the same threshold for all clinical research staff ensures consistency and fairness.
Referring back to Adams’s equity theory of motivation, the tier advancement process provides staff with direct means to see what they are getting out of the job equals what they put in. It also creates a sense of consistency that what they are putting into their job and what they get out is equivalent to that of their peers.
The competency-based tier advancement workforce initiative also meets many of Champagne and McAfee’s aspects of employee needs. It addresses “security,” both in the psychological and economic sense, by providing clear job descriptions and by employing a regular market analysis to ensure fair wages. It speaks to “affiliation” by promoting leadership; in order to advance in tiers, candidates must meet the leadership competencies appropriate for the tier toward which they are working. Leadership and professionalism inherently encourages participation in things outside “the job” that will further the clinical research community. “Esteem” and “self-actualization” are met through the development of challenging job advancement criteria with a definite outcome of achieving the next tier.
Duke will continue to focus on advancing its clinical research workforce. The framework described here is expected to be woven into the institution’s performance review process in the coming years, with the possibility that competency-based assessments will be applied to senior and management positions. By tying these expectations to existing performance and merit review processes, Duke will enhance an already established workflow rather than “reinvent the wheel.”
Conclusion
Shifting the research culture takes time. Standardizing job classifications and introducing new processes for advancement can be of great benefit to staff involved in clinical research.
The role of the clinical research professional needs to be valued, and should be more widely recognized as requiring high-level skills. Advancing the language and expectations in clinical research job classifications allows for a standardized pathway for building a career in an AMC. However, it does not guarantee this by way of tenure, but rather through demonstration of competencies.
By shifting the workforce’s expectations at Duke to competency-based advancement, the institution expects to have less attrition and more job satisfaction among staff choosing to work in clinical research. The tier advancement model has multiple advantages that are anticipated to result in a cultural shift that focuses on advancing clinical research and that leads to improved patient care and health outcomes.
References
- Meador KJ. 2015. Decline of clinical research in academic medical centers. Neurology 85(13):1171–6.
- Ramlall S. 2004. A review of employee motivation theories and their implications for employee retention within organizations. J Am Acad Bus 5(no.1/2):52–63.
- Champagne PJ, McAfee RB. 1989. Motivating Strategies for Performance and Productivity: A Guide to Human Resource Development. Quorum Books.
- Maslow AH. 1943. A theory of human motivation. Psych Rev 50(4):370.
- Adams JS. 1963. Towards an understanding of inequity. J Abnormal Soc Psych 67(5):422–36. http://psycnet.apa.org/record/1964-04111-001
- Brouwer RN, Deeter C, Hannah D, Ainsworth T, Mullen C, Hames B, Gaudaur H, McKellar T, Snyder D. 2017. Using competencies to transform clinical research job classifications. J Res Admin. In press.
- Causey M. 2017. Professional pathways boost staff retention in clinical research settings. ACRP Blog. www.acrpnet.org/2017/04/24/professional-pathways-boost-staff-retention-clinical-research-settings/
- Sonstein SA, et al. 2014. Moving from compliance to competency: a harmonized core competency framework for the clinical research professional. Clin Res 28(3:17–23. www.coapcr.org/wp-content/uploads/2014/10/Clinical-Research-Competencies.pdf
- Snyder DC, et al. 2016. Retooling institutional support infrastructure for clinical research. Contemp Clin Trials 48:139–45.
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. 2009. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Informatics 42(2):377–81.
Rebecca Namenek Brouwer, MS, (rebecca.brouwer@duke.edu) is director of research initiatives at Duke University in Durham, N.C.
Deborah Hannah, BS, (deborah.hannah@duke.edu) is research practice manager at Duke University Medical Center.
Christine Deeter, BS, (christine.deeter@duke.edu) is operations coordinator at Duke University School of Medicine.
Betsy Hames, JM, (betsy.hames@duke.edu) is senior human resources executive at Duke University School of Medicine.
Denise Clutter Snyder, MS, LDN, RD, (denise.snyder@duke.edu) is associate dean for clinical research at Duke University School of Medicine.


